
Parent FAQs
What is “sex”?
“Sex” is the biological classification of an organism according to its reproductive role. A person’s sex is determined at conception when the human ovum (egg), carrying an X chromosome is fertilized by a sperm cell carrying either an X or Y chromosome. If the ovum is fertilized by a sperm cell carrying an X chromosome, then the new human being has XX chromosomes and is female. If the ovum is fertilized by a sperm cell carrying a Y chromosome, then the new human being has XY chromosomes and is male. (Only the Y chromosome carries the Sry gene, which directs the organization of the developing human being as male; without the Sry gene, the child is female.)
The person’s chromosomes (XX or XY) direct bodily development so that, at maturity, the body is equipped to procreate. Males develop testes, which generate sperm cells, and females develop breasts, a womb, and ovaries, which produce human ova (eggs). When a child is born, the reality of the child’s sex is acknowledged, not arbitrarily “assigned.” In rare cases, something goes wrong during the child’s development in the womb, resulting in a Disorder of Sexual Development (DSD or Intersex Condition), which may make it more difficult initially to determine the child’s sex at birth. See “What does ‘intersex’ mean?” below.
From conception, then, “every cell [of the person’s body] has a sex” and a person’s sex—male or female—cannot change.1
References
1. Institute of Medicine (US) Committee on Understanding the Biology of Sex and Gender Differences; Wizemann TM, Pardue ML, editors. Exploring the Biological Contributions to Human Health: Does Sex Matter? Washington (DC): National Academies Press (US); 2001. 2, Every Cell Has a Sex. Available from: https://www.ncbi.nlm.nih.gov/books/NBK222291/
What is “gender identity”?
Every person has a sexual identity (male or female) based on biological sex. The theory that a person has a “gender identity” distinct from bodily sex was first promoted in the 1950s by Dr. John Money, a psychologist who treated transsexuals and children with disorders of sexual development. Gender identity is described as “an internal sense of being male, female or something else, which may or may not correspond to an individual’s sex assigned at birth or sex characteristics” (APA 2018).1 Gender identity is a subjective feeling, sometimes linked to a person’s sense of conformity to stereotypes or cultural norms; it cannot be tested, measured, or objectively validated. Proponents of this belief claim all gender identities, including “non-binary” or “gender-queer,” are healthy and normal and each person has the autonomy to discern or declare a unique gender identity, regardless of sex (male or female). This belief in a self-determined identity, however, creates an antagonistic relationship with the body, which is unhealthy and profoundly confusing. In contrast, the Church teaches that the person is a unity of body and soul, and that “[e]veryone, man and woman, should acknowledge and accept his sexual identity” (CCC, 2333).2
References
1. American Psychological Association. (2018). A glossary: Defining transgender terms. Monitor on Psychology, 49(8), 32. Retrieved from https://www.apa.org/monitor/2018/09/ce-corner-glossary
2. Catechism of the Catholic Church, 2nd ed. (Washington, DC: United States Catholic Conference, 2000), 2333.
What is a human being? What does it mean to be a human person?
Our faith teaches that each human being is most fundamentally a beloved daughter or son of God, created in God’s own image and likeness. God’s design for human beings includes being male or female: “in His own image, in the image of God he created them; male and female he created them” (Gen 1:27; Mk 10:6; Mt 19:4). Notice that sexual difference is simultaneous with the equal dignity of being created in God’s image.
Unlike angelic persons, who are spirits without bodies, God creates the human person to be a unity of body and soul, which means that “the human body shares in the dignity of ‘the image of God’” (CCC, 364).1 This is why the Church teaches that “man may not despise his bodily life. Rather he is obliged to regard his body as good and to hold it in honor since God has created it and will raise it up on the last day” (CCC, 364 quoting Gaudium et Spes 14).2 A person’s dignity is inalienable; it is not dependent on legal recognition, appearance, or others’ opinions. Because every person is loved by God and made for love, a person should never be treated as an object or a thing to be used.
References
1. Catechism of the Catholic Church, 2nd ed. (Washington, DC: United States Catholic Conference, 2000), 364.
2. CCC, 364.
What is “gender ideology” and what does it say about the human person?
Gender ideology is an erroneous system of beliefs about the human person, with philosophical roots in nihilism, atheism, Marxist-feminism, and queer theory. Although the beliefs proposed by gender ideology are sometimes presented as aligned with Christian compassion and human dignity, they are incompatible with the Christian view of the human person or the good of the individual person. Psychological and medical interventions based on gender ideology are causing serious harm, especially to children, adolescents, and other vulnerable persons.
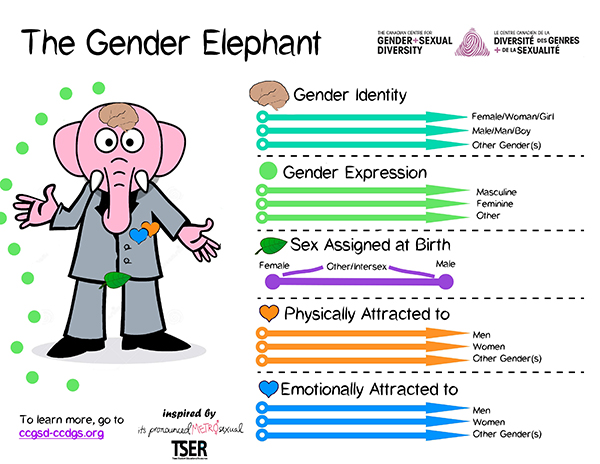
Gender ideology, unlike Christian anthropology, presents the human person as a dis-integrated, fractured being whose dimensions—described as gender identity, gender expression, sex assigned at birth, romantic orientation, and sexual orientation—are independent, need not align, and may change over time (as represented by the Gender Elephant, below, or similar images). Note that the image falsely portrays biological sex on a spectrum, as if a person could be more or less male or female, with “intersex” (disorders of sexual development) elsewhere on the spectrum. See “What does ‘intersex’ mean?” below.
In brief, gender ideology is fundamentally opposed to Catholic teachings because:
- It is essentially atheistic or at least agnostic: It fails to acknowledge the Creator and our radical dependency on Him, and instead elevates personal autonomy and self-determination. (Not all who accept gender ideology are atheists or agnostics. Some believers are unaware of its incompatibility with Christianity.)
- It rejects the truth that the human person is a unity of body and soul, made in the image and likeness of God, with a given nature.
- It claims that each person determines his or her identity according to personal desire or choice, regardless of objective bodily reality.
- It views the body as a tool or thing to be used in the expression of human will and rejects the idea that the body has an intrinsic, objective meaning that sheds light on who we are.
- It denies sexual difference (male or female) and rejects the idea that the body is a gift from our Creator.
- It “enforce[s] the false idea—that a man can be or become a woman or vice versa…” (USCCB, “Created Male and Female,” 2017). Gender ideology also promotes the false idea that a person can deny his or her sexual identity (male or female) and assert a “non-binary” or other identity at odds with biological sex.
What do “transgender” and “nonbinary” mean?
The term “transgender” is used by advocacy groups as “an umbrella term encompassing those whose gender identities or gender roles differ from those typically associated with the sex they were assigned at birth.”1 Activists similarly describe people who identify as “nonbinary” as being “born with bodies that may fit typical definitions of male and female, but their innate gender identity is something other than male or female.”2 The common thread is that persons who identify as transgender or nonbinary or something else reject their sexual identity as male or female in favor of a self-determined identity.
The Church teaches that everyone must accept his or her sexual identity as a gift from our Creator (CCC, 2333).3 Scientifically, it is not possible for a person to “be” or become the opposite sex. No person should repudiate his or her sexual identity by asserting a transgender, non-binary or gender fluid identity. Catholics should avoid language that appears to support the idea that a person can “be” something other than male or female, or that suggests people are defined by their feelings or desires. Instead of saying a person “is” transgender or nonbinary, it is more accurate to describe the person as a “person who identifies as transgender” or as a “transgender-identified person.”
Pastoral and professional care for persons struggling to accept their sexual identity should aim to harmonize their subjective experiences with their objective biological reality (male or female). For some people, therapy to address past trauma or underlying mental health issues may prove helpful. It is also important to affirm that there are many different ways to flourish as a man or a woman; the rejection of overly rigid sex roles does not entail a rejection of sex itself. See “What about a person who has interests, preferences, or behaviors typically associated with the opposite sex?” below.
References
1. “A Glossary: Defining Transgender Terms.” Monitor on Psychology 49, no. 8 (September 2018): 32. https://www.apa.org/monitor/2018/09/ce-corner-glossary.
2. “Understanding Non-Binary People: How to Be Respectful and Supportive.” National Center for Transgender Equality, October 5, 2018. https://transequality.org/issues/resources/understanding-non-binary-people-how-to-be-respectful-and-supportive.
3. Catechism of the Catholic Church, 2nd ed. (Washington, DC: United States Catholic Conference, 2000), 2333.
Can a person be “born in the wrong body”? What is gender dysphoria?
Sometimes children, adolescents, or adults experience feelings of dislike for their bodies or feel like their bodies are “wrong” or don’t “fit” who they are. These feelings may persist in ways that interfere with a person’s functioning. This “disconnect” between objective reality and a person’s subjective self-perception is common to a number of psychological conditions (e.g. anorexia nervosa, body integrity identity disorder, body dysmorphia). The sources of these various disorders are complex and not very well understood.
Until recently a person expressing a sense of being “in the wrong body” would have been understood as suffering a similar psychological disorder and in need of treatment to help align self-perception with objective reality. This phenomenon was described as gender identity disorder (GID) in the Diagnostic and Statistical Manual of Mental Disorders III (DSM-III) and listed as a mental health diagnosis in the DSM-IV of 1994.
In 2013, the DSM-V replaced GID with a new diagnosis, gender dysphoria, that characterizes a person’s distress over an identity at odds with biological sex as pathological but validates the underlying identity as normal.1 In 2019, the World Health Organization classified this experience as “gender incongruence,” describing it as a normal human variation to be affirmed and, if desired, supported with medical or surgical interventions to align the body’s appearance with the desired identity.2
In other words, over a short period of time and under social and political pressure, medical and psychological organizations have radically shifted their treatment approach towards anyone who asserts an identity at odds with biological sex. They no longer treat a perceived mismatch between body and identity as a psychological disorder requiring psychological treatment, but as a normal human variation that deserves validation and “on-demand” medical interventions to modify the body to match the person’s felt-identity. This change is not supported by sound psychology or medical research. From the Catholic perspective, the truth about the human person as a body-soul unity is non-negotiable. Catholics can neither support the view that a person is born “in the wrong body” nor facilitate medical or surgical body modifications as a remedy for distress over sexual identity or as an expression of personal autonomy. (Gender dysphoria is different from the situation of a person with a Disorder of Sexual Development/Intersex condition. For more information see “What does ‘intersex’ mean?” below.)
References
1. Diagnostic and statistical manual of mental disorders: DSM-5. Arlington, VA: American Psychiatric Association. https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM-5-Gender-Dysphoria.pdf
2. International Statistical Classification of Diseases and Related Health Problems (11th ed,; ICD-11; World Health Organization, 2019). https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f90875286
What does “intersex” mean?
“Intersex” is the informal description for conditions diagnosed as Disorders of Sexual Development (DSD). These rare conditions occur during fetal development and may include chromosomal, hormonal, or organ abnormalities. Research indicates that the impact of a DSD varies greatly, ranging from minor effects diagnosed later in life to serious anomalies causing infertility or requiring immediate surgery or lifelong hormonal treatment. Among the most common “intersex” disorders are: Klinefelter Syndrome, affecting an estimated 1 in 500-1000 males; Congenital Adrenal Hyperplasia, affecting an estimated 1 in 10,000 to 15,000 live births, impacting males and females in significantly different ways; and Androgen Insensitivity Syndrome, affecting an estimated 1 in 99,000 males.1,2,3
Transgender activists and proponents of gender theory often cite DSDs as evidence that sex is not binary (male or female). They argue that intersex disorders “prove” the existence of a “third sex” or that sex exists on a “spectrum.” This is nonsense. A disorder of sexual development is not evidence of a “spectrum” of normal sexual identity any more than a defect in the development of the heart is evidence of a “spectrum” of normal heart structures. Medical or surgical interventions to address intersex conditions can be legitimate means to restore the body’s healthy functioning. Some persons born with DSD rightly protest the treatment protocol developed decades ago under the influence of Dr. John Money. He maintained that a child’s identity was not innate but dependent on socialization; thus whether and what kind of surgery to perform on the genitals of a child with DSD would be decided not on predominant chromosomal makeup or optimal bodily function but on the basis of which genitals (male or female) would be easiest to surgically construct. Such surgeries often caused harm, both physical and psychological. Unlike a person with DSD, a person who identifies as transgender and seeks a “gender transition,” using medical or surgical interventions to modify the body, has a healthy body to begin with. Taking hormones or having surgery as part of a gender transition damages or destroys the healthy body and is not morally permissible.
References
1. “Klinefelter Syndrome.” NORD (National Organization for Rare Disorders), 2017. https://rarediseases.org/rare-diseases/klinefelter-syndrome/.
2. “Congenital Adrenal Hyperplasia.” NORD, 2018. https://rarediseases.org/rare-diseases/congenital-adrenal-hyperplasia/
3. “Partial Androgen Insensitivity Syndrome.” NORD, 2019. https://rarediseases.org/rare-diseases/androgen-insensitivity-syndrome-partial/
What do people mean by “gender transition”?
The term gender transition is a catch-all phrase that describes different steps a person might take to modify external appearances to reflect the desired “gender identity.” A social transition can include changes in clothes, hair, and behavior to assert an identity that differs from the person’s biological sex. A medical transition involves off-label use of medication to block the normal process of puberty or to induce the development of secondary sex characteristics of the opposite sex. Surgical transition involves surgery to remove reproductive organs or genitals, create a “neovagina” or “neophallus” (simulated genitals), or modify the body’s appearance in other ways.1,2 A legal transition occurs when a person changes his or her name or sex on legal documents such as a birth certificate or passport.
In reality, however, a person cannot actually “transition” to “become” someone other than the male or female person God created them to be. The Catholic Church, supported by reason and science, teaches that a person’s sex (male or female) is innate (from conception) and immutable. A so-called “gender transition” is premised on the erroneous theory that a person can reject his or her sexual identity (male or female) and assert a self-defined “gender identity” at odds with bodily reality. This is harmful and not conducive to human flourishing.
Social, medical, and surgical interventions to facilitate a person’s “transition” actually pathologize healthy bodies, disrupt natural developmental processes, and carry serious lifelong consequences. For example, a child who “transitions” using puberty blockers followed by cross-sex hormones as an adolescent becomes infertile forever. The medical and surgical interventions now used to affirm a child or adolescent’s gender identity amount to dangerous medical and psychological experiments, based on scant, low-quality evidence, with little research on long-term effects or medical harm. Neither adolescents nor the parents of children or adolescents undergoing transition procedures can give meaningful informed consent, because the long-term complications and consequences of these interventions are unknown.
It is neither compassionate nor loving to support or affirm a person’s desire to transition. Accommodating a person’s “transition,” at any stage, validates the person’s false belief that it is possible to have an “authentic” identity that contradicts bodily reality. Even a child’s social transition, however minimal, is harmful because it conveys adult approval of the child’s desired identity and reinforces the child’s false belief that he or she really “is” someone other than the male or female God created. See below for FAQs on specific “stages” of “transition.”
References
1. Dreher, P. C., Edwards, D., Hager, S., Dennis, M., Belkoff, A., Mora, J., Tarry, S., & Rumer, K. L. (2018). Complications of the neovagina in male-to-female transgender surgery: A systematic review and meta-analysis with discussion of management. Clinical anatomy (New York, N.Y.), 31(2), 191–199. https://doi.org/10.1002/ca.23001
2. Frey, J. D., Poudrier, G., Chiodo, M. V., & Hazen, A. (2016). A Systematic Review of Metoidioplasty and Radial Forearm Flap Phalloplasty in Female-to-male Transgender Genital Reconstruction: Is the “Ideal” Neophallus an Achievable Goal?. Plastic and reconstructive surgery. Global open, 4(12), e1131. https://doi.org/10.1097/GOX.0000000000001131
What is “gender affirmative care”?
The premise of “gender affirmative care” or “gender affirmation” is that all “gender identities” are normal and healthy, and that gender identity and expression are “basic human rights.” According to The Gender Affirmative Model,1 “gender may be fluid, and is not binary, both at a particular time point and if and when it changes within an individual over time.” Advocates of the gender affirmative model say that every child should have the “opportunity to live in the gender that feels most real or comfortable to that child and to express that gender with freedom from restriction, aspersion, or rejection.” This approach tells parents, professionals, and others to encourage gender “exploration” and to affirm a child or adolescent’s asserted gender identity, regardless of whether it aligns with the person’s biological sex. Although research shows that children and adolescents identifying as transgender or nonbinary are significantly more likely than their peers to have serious mental health issues, the affirmative care model attributes “any pathology” to “cultural reactions to gender diversity” rather than to underlying mental health disorders. Although the gender affirmative model is heavily promoted by several U.S. medical associations and by physicians who specialize in gender transitions, it is highly controversial and not well-accepted internationally. (In April 2020, the U.K. announced plans to prevent minors under 18 from taking “gender-affirming” hormones.) “Gender-affirming care” is unsupported by quality scientific research and is incompatible with the Catholic view of the person.2
As Catholics, we affirm each person’s unconditional dignity and value, which come from being loved by God and formed in God’s image and likeness, but we cannot affirm a person’s “transition” or an asserted gender identity in opposition to the person’s sex. True affirmation acknowledges not only the person’s inherent dignity but also the truth of their situation—their unchangeable identity as male or female. Even if well-intended, “affirmative care” is not an authentic expression of care and compassion, as it denies the truth and is not oriented towards the genuine good of the person.
References
1. The Gender Affirmative Model: An Interdisciplinary Approach to Supporting Transgender and Gender Expansive Children, C. KeoMeier and D. Ehrensaft (Editors) American Psychological Association (2018).
2. Malone, William J., Gender Dysphoria Resource for Providers, 3rd edition (2019).
What is “conversion therapy”?
The phrase “conversion therapy” is an imprecise umbrella term that originally was applied to a wide range of psychological interventions for persons experiencing same-sex attraction. The term fails to distinguish traditional talk therapy that explores, at the client’s request, unwanted feelings of sexual attraction or behavior from unethical, coercive practices of the past, which tried to force “change” in a person’s sexual orientation. In recent years, several states have passed “conversion therapy” laws that not only restrict talk therapies for same-sex-attracted clients but also restrict talk therapies for clients, including minors, who are experiencing identity issues. These “conversion therapy bans” attempt to dictate the goals of therapy by permitting only therapy that affirms LGBTQ identities and behaviors, while preventing therapists and their clients from exploring underlying reasons for a person’s feelings in hopes of resolving them. These laws not only impose a one-size-fits-all approach to therapy, but also restrict the free speech and religious rights of both therapists and clients. It is particularly damaging for children and adolescents to be denied sound psychological treatments to help them accept their bodies, integrate feelings with sexual identity, and find healing for underlying traumas or wounds. And it is unconscionable for the government or gender experts to dictate the use of gender-affirming therapies on children and adolescents, and effectively consign those who transition to lives characterized by medical dependency, mental health diagnoses, and elevated risks of suicide.
It is critically important to note that there is no scientific evidence that psychological interventions to help a child accept his or her bodily sex are harmful. In fact, research shows that children experiencing identity confusion or “gender dysphoria” typically resolve those issues with therapy that addresses underlying psychological issues or family dysfunction, or even with no treatment at all.1 Activists sometimes claim that research has shown that “conversion therapy” to help a child or adolescent accept his or her biological sex is harmful. This is completely false, as no research has ever shown that therapies to help children or adolescents integrate their feelings with their biological sex are harmful. Further, no research has even been conducted regarding the relative harm or success of gender-affirming therapy versus talk therapy (erroneously described as “conversion therapy”) to help children or adolescents experiencing “gender identity” issues. Past research evaluating “conversion therapy” pertained only to the outcomes of specific treatments for sexual orientation in adults, not “gender identity” in children. Unfortunately, these “conversion therapy” bans are part of a larger ideological campaign to change our cultural beliefs about the human person, replacing the truth that we are created by God as male or female, forever, with the lie that each person is self-defining and all “gender identities” are normal and healthy.
References
1. Steensma, T. D., Mcguire, J. K., Kreukels, B. P., Beekman, A. J., & Cohen-Kettenis, P. T. (2013). Factors Associated with Desistance and Persistence of Childhood Gender Dysphoria: A Quantitative Follow-Up Study. Journal of the American Academy of Child & Adolescent Psychiatry,52(6), 582-590.
What about a person who has interests, preferences, or behaviors typically associated with the opposite sex?
Many people – children, adolescents and adults – have interests or mannerisms that may be stereotypically associated with either males or females. But stereotypes are just that—stereotypes. They reflect something about reality by describing “typical” behavior, but stereotypes should not be used to define what is “normal.” Nor should they be viewed as rigid boundaries on human behavior. Stereotypes also cannot predict individual interests or behaviors. This helpful graph illustrates this point:
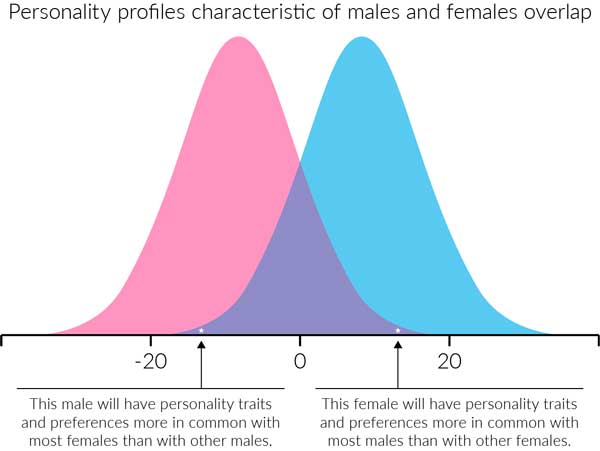
Image based on Malone, et al, Quillette (2019)
This graph shows results of recent research that looks at human personality traits and maps these by sex (male and female); the research studied males and females in the US and other developed countries where there is freedom for individuals to embrace their interests and preferences independent of rigid cultural norms.1 The research found significant overlap between the personalities and preferences of males and females. Although males tend to have more in common with other males (as represented by the blue areas in the graph), because of the overlap between males and females, some males (represented by the dot at the left of the blue curve) actually have more personality traits and preferences in common with most females than they do with other males. The same observation holds true for females.
So what does this mean for children and adolescents? Given the current false narrative that someone could have a “gender identity” different from biological sex, a girl who happened to have a lot in common with boys “could be led to incorrectly conclude that she is really a male, born in the wrong body. That child’s parents could become confused as well, noticing how ‘different’ their child’s behavior is from their own, or from that of their peers. In reality, that child simply exists at the end of a behavioral spectrum, and ‘sex-atypical’ behavior is part of the natural variation exhibited both within and between the sexes” (Malone et al, 2019). In fact, “personality and behavior do not define one’s sex” (Malone et al, 2019) so allowing stereotypes to dictate identity, as advocated by gender theory and the Affirmative Care model, will confuse children about what it means to be male or female, and make them less free to pursue their own interests and express their own unique personalities.
References
1. Graph adapted from: Malone, W. J., Wright, C. M., & Robertson, J. D. (2019, September 24). No One Is Born in ‘The Wrong Body’. https://quillette.com/2019/09/24/no-one-is-born-in-the-wrong-body/. The research on personality is presented in Kaiser, T, Del Giudice, M, Booth, T. Global sex differences in personality: Replication with an open online dataset. Journal of Personality. 2019; 00: 1– 15. https://doi.org/10.1111/jopy.12500
What is “social transition”?
A person who rejects his or her sexual identity (male or female) and desires to assert a new “gender identity” at odds with biological sex often begins a “social transition” as the first step in a “gender transition.” Social transition is a process of adopting the external appearance of the desired sex or, in the case of someone who desires to identify as non-binary, rejecting the appearance of one’s biological sex. A person who embarks on social transition chooses clothing, hair styles, names, pronouns, and expressive behavior to project the appearance of the desired identity. The person making a social transition wants others to “see” and validate this new “gender identity”: others are expected to call the person by a chosen name or pronouns, to allow the person to use the restrooms or private spaces reserved for members of the opposite sex, and to convey approval and support for the person’s asserted identity. Other people are expected, and increasingly required, to affirm the “gender identity” expressed in a social transition.
Social transition cements the child’s alienation from his or her own sexual identity, as adults affirm the child in rejecting his or her biological sex. Moreover, the process of social transition requires the one who transitions, and everyone else, to affirm continually an identity that is not and cannot be true. A person who socially transitions may experience increased anxiety, wondering whether others “see” and accept their desired identity. When others validate the person’s desired identity—affirming the social transition as if the person really has become someone other than the male or female God created them to be—they implicitly affirm the fundamental premise of gender ideology: that a person can self-determine “who they are,” regardless of biological sex. Catholics cannot affirm a social transition, which is a rejection of a person’s God-given sexual identity.
What about puberty blockers?
The Affirmative Care model promotes the practice of treating prepubescent children who question or express confusion about their identity with medicines called GnRH agonists or “puberty blockers.” These medicines, which stop the normal processes of puberty, are prescribed when the child reaches Tanner Stage 2, as he or she begins to show signs of maturation, but before the development of secondary sex characteristics. Puberty blocking medications are FDA approved only as a treatment for precocious puberty; their use in treating gender dysphoria (where the body is healthy and developing normally) is an off-label use. Although they are promoted as harmless and reversible (like pressing a “pause” button), puberty blockers can have serious consequences, including decreasing bone density and arresting bone growth, hindering normal maturation and brain organization, and blocking the development of the child’s reproductive organs and gametes (sperm and ova). The use of puberty blockers sometimes increases the child’s feelings of not fitting in with peers: the physical immaturity of the “blocked” child creates a gulf between the child and the child’s peers who are progressing through normal puberty.
The Catholic Church teaches that it is unethical to use medication to induce a diseased state in a healthy body. Prescribing puberty blockers induces a diseased state (hypogonadotropic hypogonadism) in which the normal development of the body is blocked from proceeding. In addition, the long-term physical consequences of using puberty blockers are unknown. Instead, each child should be helped to accept his or her body and sexual identity as a gift, while still understanding each person is an individual, free to express a unique personality.
What about cross-sex hormones?
In “gender-affirming” care, the administration of cross sex hormones to a child follows administration of puberty blockers, but it also can be the initial step of medically transitioning an adolescent or adult. Cross-sex hormones such as estrogen or testosterone are used off-label in order to induce the appearance of secondary sex characteristics of the opposite sex.1 Males use female hormones such as estradiol (often along with anti-androgens to reduce testosterone) in order to modify the body to appear more feminine. Females use testosterone to modify the body to appear more masculine. A person who identifies as non-binary might receive low levels of cross-sex hormones to create an ambiguous appearance. Gender-affirming protocols call for cross-sex hormones to be administered at 16, but increasingly advocates promote the use of cross-sex hormones at earlier ages. In fact, the protocol for an observational study funded by the NIH expressly states that cross-sex hormones were used on at least one child at age 8.2 Changes induced by cross-sex hormones, including changes to voice, hair and genitals (atrophying or shrinking) are irreversible; even worse, the combination of puberty blockers and cross-sex hormones leads to sterility. Use of these hormones comes with many associated health risks, including venous thromboembolic events, metabolic syndrome and abnormal lipid profiles, and decreases in bone density. Moreover, physicians have noted that use of cross-sex hormones often increases, rather than resolves, distress about the body, and the risk of suicide remains (see “What about suicide?” below). The Catholic Church teaches that mutilation of a healthy body either surgically or hormonally is never permissible. Cross-sex hormones involve modifying a healthy body to project an appearance that denies the gift of one’s sexual identity and seeks to create the appearance of an identity that is untrue.
References
1. Cavanaugh, T. Gender Affirming Hormone Therapy. National LGBT Health Education Center, Fenway Institute. Retrieved from https://fenwayhealth.org/wp-content/uploads/Friday-Session-5a.pdf
2. Olson-Kennedy, J., et al. (2019). Impact of Early Medical Treatment for Transgender Youth: Protocol for the Longitudinal, Observational Trans Youth Care Study. JMIR Research Protocols, 8(7). doi: 10.2196/14434
What about surgical transition?
Surgical transition involves body modifications that include “top surgery” (mastectomies), “bottom surgery” (removal of the genital and reproductive organs), and surgical reconstruction of the genital area to construct neo-genitals or change its appearance in other ways. Additional surgical modifications include facial feminization surgery and surgical voice modification. Both top and bottom surgeries are offered at increasingly younger ages, with mastectomies performed on females as young as 13, and bottom surgery increasingly performed on males as young as 16. These surgeries can have serious complications, and often require repeat surgeries and hospitalizations. The suicide rates remain high even after surgical transition.
According to Catholic teaching, it is never permissible to mutilate a healthy body. Moreover, surgical transition seeks to destroy the gift of one’s sexual identity by mutilating the body in order to create an appearance that differs from one’s sexual identity. Genital surgeries typically destroy the capacity for reproduction and amount to intentional sterilization. Direct sterilization procedures also are not permissible and are gravely unethical.
What does the Church say about “accompanying” others in these situations?
Pope Francis has repeatedly stressed the importance of accompanying and not abandoning persons who identify as transgender or who struggle with gender dysphoria. Accompaniment means walking with others, in charity and truth. As US Bishops Bambera, Chaput, Conley and Kurtz noted in a joint statement, “a person’s discomfort with his or her sex, or the desire to be identified as the other sex, is a complicated reality that needs to be addressed with sensitivity and truth. Each person deserves to be heard and treated with respect; it is our responsibility to respond to their concerns with compassion, mercy and honesty” (“Created,” 2017).1
At the same time, these bishops stressed, it is essential to help individuals who identify as transgender or who are diagnosed with gender dysphoria to accept their sexual identity, by coming to accept the body as a gift from God. Charity is inseparable from the truth. Even if well intentioned, it is a false charity to affirm another person’s rejection of the truth. The human person finds happiness only in the light of truth. Because the Church desires “the health and happiness of all men, women, and children,” the Bishops wrote, “we call for policies that uphold the truth of a person’s sexual identity as male or female, and the privacy and safety of all. We hope for renewed appreciation of the beauty of sexual difference in our culture and for authentic support of those who experience conflict with their God-given sexual identity.” Family and friends are encouraged to reassure transgender-identified persons of their inherent dignity and infinite value, and to support them, with love, on the path towards full acceptance of their bodies and integration of their male or female identity.
References
1. “Created Male and Female: An Open Letter from Religious Leaders,” released on December 15, 2017. http://www.usccb.org/issues-and-action/marriage-and-family/marriage/promotion-and-defense-of-marriage/created-male-and-female.cfm
What about pronouns?
Persons who identify as transgender or nonbinary often choose to disclose their asserted identities by using new personal pronouns that do not match their biological sex. Further, transgender or nonbinary-identified persons typically enlist others’ participation in these new self-narratives, insisting that others validate their self-determined identities by addressing them by their chosen pronouns. In some places, anti-discrimination laws or business practices seek to require others’ compliance with the requested pronoun changes. Activists argue that using the pronouns chosen by transgender-identified persons is simple courtesy and kindness, and that failing to use chosen pronouns is discriminatory and causes harm by “invalidating” the person’s asserted identity or worsening the person’s dysphoria.
These arguments fail to acknowledge that personal pronouns have an objective meaning. They signify a fact: the person’s sex as male or female. When chosen pronouns are at odds with a person’s biological sex, then those pronouns effectively “tell a lie” about who the person is (male or female). By choosing new personal pronouns at odds with biological sex, a transgender or nonbinary-identified person communicates rejection of his or her sexual identity in favor of a new, self-determined identity. He or she communicates something that is not objectively true (e.g., a male who calls himself “she” is falsely claiming to be female). Even if transgender-identified persons sincerely believe that they “are” the people they feel themselves to be, regardless of biological sex, it is not right to validate that false belief. Charity and truth cannot be separated. While it is compassionate to be sensitive to someone else’s distress, it is a false compassion to affirm someone’s rejection of his or her sexual identity. In addition, it is particularly harmful to transgender-identifying children or adolescents for their parents or other adults to affirm, through the use of chosen pronouns or names, their false belief in an identity that rejects the reality of biological sex. Instead, each person must be helped to accept his or her sexual identity (male or female) and to discover that the true source of dignity and self-worth lies in God’s unconditional love, not in “validations” from others.
Government or institutional policies that require others to use the chosen pronouns of a transgender-identified person are problematic for several reasons. These policies compel speech by forcing others to speak words they do not want to say or which they believe are not true (for example, requiring a person to use “she” to reference a biological male although “she” applies to females). In addition, pronoun policies also may violate the conscience and religious freedom rights of those whose faith compels them to speak the truth and to affirm, rather than deny, the reality that God made human beings as male or females, forever.
In workplace settings, or to avoid distressing a transgender-identified adult over pronouns, it may be helpful to address the person directly by name whenever possible, avoiding pronouns. This may help minimize the risks of misunderstandings, hurt feelings, or employment issues.
What about using someone’s new “chosen” name?
Often a person who identifies as transgender or nonbinary will announce a new name in the process of disclosing that identity. He or she typically asks others to use this new name in place of the previous name, to signify the shift in identity. Whether the person identifying as transgender or nonbinary is an adult or an adolescent or child will likely play a role in determining the right response. In general, using chosen names is not recommended for children or adolescents who are experiencing identity issues. Whenever parents, peers, or other adults use the name specifically chosen by the child or adolescent to express a self-determined identity at odds with biological sex, they reinforce the child or adolescent’s false beliefs. It is especially important for children and adolescents to hear a consistent message from the adults in their lives about the truth of who they are (male or female) and their infinite value in the eyes of God and the hearts of those who love them. It is helpful to realize that children or adolescents asserting new “trans” or “nonbinary” identities may appear more certain about the new identity than they really are.
More and more young people who previously identified as transgender or nonbinary are “de-transitioning” (reclaiming their sexual identities), often after undergoing medical or surgical transitions. These de-transitioners often express their disappointment that parents, physicians and counselors quickly validated their new identities and facilitated their transitions and related medical interventions. They ask, after the fact, why no one tried to stop them and why no one asked why they were rejecting their biological sex. Keira Bell, for example, sued the Tavistock Clinic in London for not adequately investigating underlying causes of her dysphoria. “I should have been challenged on the proposals or the claims that I was making for myself,” she lamented.1 Unfortunately, parents face a tremendous amount of pressure from counselors and trans advocates to embrace the child’s new identity by accepting the chosen name and identity. Some parents worry that refusing to go along with the chosen name and intended transition may be cast as unsupportive or abusive and lead to their child being removed from the home.
When the person identifying as transgender or nonbinary is an adult, the situation is different. Adults in general—regardless of whether they assert a transgender identity or not — have the legal right (and presumably the maturity) to make decisions about how they would like to be addressed by others, including whether to seek changes to legal names. In situations involving adults, the decision about using a chosen name may be affected by the relationship to the person requesting the chosen name. Family members, for example, might judge that using a chosen name reinforces the transgender identity and undercuts their efforts to help their loved one come to accept his or her sexual identity. On the other hand, at work, many people worry that failure to use a colleague’s chosen name could be deemed workplace harassment or insubordination and become grounds for dismissal. In the public square, it is courteous to address other adults as they introduce themselves to you, without making judgments about whether the name matches someone’s sexual identity. In sum, with adults, the decision to use someone’s chosen name is a matter of prudence that should be guided by charity and determined by the closeness of one’s relationship.
References
1. Holt, A. (2020, March 1). NHS gender clinic ‘should have challenged me more’ over transition. Retrieved from https://www.bbc.com/news/health-51676020
What is “LGBTQ”? How is sexual orientation related to “gender identity”?
“LGBTQ” stands for “lesbian, gay, bisexual, transgender, and queer.” It is often assumed that people who self-identify using one of these labels belong to a community with uniformly shared goals, needs, and concerns. The reality is more complex.
The concept of sexual orientation, which expresses sexual attraction, affirms the reality of biological sex and includes a variety of measurable research variables, such as attraction or behavior. The belief in “gender identity,” which is central to the notion of a “transgender” identity, repudiates the reality that sex (male or female) is integral to who we are, in favor of a self-determined identity based on subjective feelings.
The significance of sexual difference (male or female) has become a source of deep division between some females, including those who identify as lesbian or bi-sexual, and some males who identify as transgender women. Females who insist on the right to female-only spaces also insist that males, no matter how much they “feel like” they are women, cannot define themselves as “women.” However, males who identify as “transwomen” and are attracted to females often insist that they are not only “women” but also “lesbians,” because they redefine same-sex sexual orientation to include attraction based on self-identified gender (e.g., attraction to a person of the same “gender”). Many females, including self-described radical feminists who identify as lesbian or bisexual, warn that concessions to transgender activists threaten decades of hard-won protections and advances on behalf of women (females). When transgender activists seek to erase “sex” as a meaningful category, they effectively erase “women” as a meaningful category as well.
Another area of competing concerns involves “gender-affirming care.” According to the DSM-V, children may be diagnosed with “gender dysphoria” if they feel unhappy about their bodies or show preferences, desires, or interests in the clothes, toys, or activities stereotypically associated with the other sex. Before “gender affirmative” theories took hold, some studies suggested a possible link between childhood identity issues and the person’s later sexual orientation as an adult: a child who experienced “gender identity” issues which resolved by puberty often subsequently expressed a same-sex sexual orientation as an adult. However, “gender-affirming” clinicians and parents now encourage such children to socially transition early on, followed by medical transition at puberty. This fast-track to transition has been divisive. Some parents, clinicians, and “LGB”-activists condemn “gender-affirmation” of children and adolescents as a kind of “conversion therapy” or “gay eugenics” targeting those who do not fit sex stereotypes and who otherwise might have identified as “gay, lesbian, or bisexual” in adulthood, and instead putting them on a pathway towards a transgender identity and lifelong medical dependence. As the “gender-affirming” approach has become more common, the number of adolescent females identifying as “transgender males” has spiked– teenage females are now about three times more likely than males to identify as transgender. This trend is disturbing to many, including some outspoken lesbian-feminists, and raises the question of whether the cultural weight of sexual abuse, violent pornography, sexual objectification of women, and adolescent ambivalence over same-sex attraction has become so toxic that it leads vulnerable adolescents to reject their female identities.
On a political level, powerful identity-based (“LGBTQ”) coalitions have driven major changes to laws governing sexual behavior, reproduction, family life, health care, education, and employment. These changes affect all Americans. In the years preceding the Supreme Court’s Obergefell decision legalizing “same-sex marriage,” groups like the Human Rights Campaign Foundation focused largely on advocacy for persons identifying as gay, lesbian or bisexual. After the Obergefell decision, transgender-identified activists who had campaigned for “same-sex marriage” demanded reciprocal support from “LGB” activists for an all-out push to normalize transgender identities and protect “gender identity” alongside sexual orientation. This alliance has been cemented for political purposes by leading LGBTQ organizations, but some dissension persists in the face of increasingly radical demands by transgender activists.
The political alliance that lumps “LGB” together with “T” and “Q” may create confusion among Catholics because it papers over significant differences in the underlying anthropology of a person who experiences same-sex attraction versus a person who rejects his or her sexual identity as male or female. The Church’s teachings regarding these situations account for the underlying differences. A person who asserts a transgender or non-binary identity rejects his or her own body and sexual identity, instead of accepting them as a gift from God. This is very different from a person who accepts his or her body but who experiences sexual attraction to persons of the same sex.
The Catechism of the Catholic Church affirms the dignity of all persons—no matter what—because human dignity is rooted in the truth that each person is created by God in his image and likeness and loved unconditionally. Every person is called to accept the truth about who we are: we are created male or female; our bodies are gifts from God; each person must accept his or her sexual identity; all persons are called to chastity—the integration of their sexuality—and to recognize that “sexuality affects all aspects of the human person in the unity of his body and soul. It especially concerns affectivity, the capacity to love and to procreate…” (CCC, 2332).
In general, the resources provided by the Person and Identity Project do not address questions related to same-sex attraction. The Person and Identity Project has been established to help Catholics understand “who we are” according to Christian anthropology and to equip Catholics to respond with truth and compassion to the pastoral challenges presented by gender ideology, particularly on questions of “sex” and “gender identity.” Catholic ministry toward persons who experience same-sex attraction, and their families, has for many years been faithfully and compassionately carried out by Courage International. We highly recommend Courage’s resources to individuals experiencing same-sex attraction and their families. Catholics also need to be aware that there are several groups that falsely hold themselves out as representing a Catholic approach to supporting persons with same-sex attraction or who identify as transgender.
How did these ideas spread so quickly through our culture? How are kids in particular learning about this?
Many American parents have expressed dismay at how quickly their children seem to have become supportive of the LGBTQ political movement and how readily they dismiss concerns about harmful effects of gender transitioning. These changes in attitudes and even behavior result from targeted advocacy and strategic campaigns promoting gender ideology through media, big business, education, healthcare, and entertainment in the US and Western Europe. Video and digital content not only have normalized same-sex relationships and behavior but also have celebrated “brave transgender kids” who “come out,” and glamorized drag queens and queer identities. Even parents who successfully shield their children from LGBTQ advocacy through the media discover that their children are being taught the vocabulary and basic beliefs of this ideology at school. Public schools in the US, Canada, and the UK increasingly present gender ideology as fact, and encourage children, from the earliest grades, to accept any expressed sexual orientation or gender identity as normal and healthy. Although some states permit parents to exercise an “opt-out” to shield their children from explicit sex education, states generally do not permit parents to exercise an “opt-out” to shield their children from the promotion of gender ideology. More to the point, it is impossible to “opt-out” of school culture and public-school culture today explicitly affirms all “sexualities and gender identities” as normal. Public schools may emphasize to parents that teaching about gender identity is meant to foster tolerance and acceptance for all, and that it has nothing to do with sex education or sexual orientation. However, presenting a belief in “gender identity” as the self-determined basis of a person’s identity, regardless of biological sex, distorts a child’s understanding of his or her body, the significance of sexual difference (male or female), and the connection between body, fertility, and family. In sum, it is at odds with science and presents as fact an erroneous vision of the human person.
Where do I find help?
Download our Counseling Resources guide.